Conditions and Treatments
Learn more about the conditions treated at Leeds General Surgery and the different treatment pathways available.
Gallstones:
The gallbladder is a pear shaped organ sitting under the liver. It is just below the ribs on the right side of the abdomen. It is a reservoir for bile, squeezing and forcing bile into the gut upon eating. Bile itself is important for digestion, as it helps to breakdown fat into smaller molecules, allowing for better absorption.

Gallstones are formed in the gallbladder, likely due to bile stasis. They can be formed of bile pigment, Cholesterol, or a mixture of both. Gallstones are present in 15-20% of people, yet only 10-15% of those people are symptomatic. Many people find out they have gallstones, incidentally through scans. Not everyone with gallstones requires intervention.
Gallstones are best seen on an abdominal ultrasound scan. They can sometimes be seen on a CT scan. Sometimes, doctors will request an MRI scan to look at the gallbladder and bile duct in more detail. In some instances, an endoscopic ultrasound (EUS) is the best test to look at the gallbladder and bile ducts.
Gallstones have three main complications.
- Biliary Colic
- Cholecystitis
- Pancreatitis
Biliary colic is a result of the gallbladder squeezing against gallstones and can cause upper abdominal pain, typically in the centre and right side of the upper abdomen, radiating into the back. The pain can be extremely intense, requiring strong pain killers. These episodes of pain can last a few minutes to a few hours. The only way to stop these attacks is an operation to remove the gallbladder.
Cholecystitis is an inflammation and/or infection of the gallbladder. This can give upper abdominal pain, a feeling on unwell, and temperatures. Patients with these symptoms should seek a medical review and are usually commenced on antibiotics. Cholecystitis is usually an indication to have the gallbladder removed, but this depends on several factors and should be discussed with a gallbladder surgeon.
Pancreatitis is a condition whereby the pancreas becomes inflamed. There is a chemical reaction within the pancreas, leading to inflammation. This can be mild, or very severe, needing treatment on intensive care. Gallstones and alcohol account for over 80% as the cause of pancreatitis. If gallstones are found in someone with pancreatitis, the recommendation is for them to have the gallbladder removed as soon as possible in order to prevent another attack of pancreatitis.
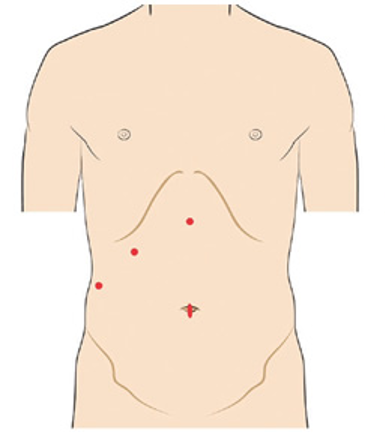
The operation to remove the gallbladder is a keyhole procedure performed under a general anaesthetic. Once the patient is asleep and on the operating table, a small cut is made near the belly button. A camera is then placed inside the abdomen, and some gas put in the abdomen in order to make space for further instruments. Three more cuts are made as shown in the diagram, and instruments are placed inside the abdomen.
The gallbladder is dissected from the liver and the correct structures are identified safely, and then the artery to the gallbladder and the duct from the gallbladder to the bile duct are clipped and cut away. The gallbladder is then taken off the liver, placed into a bag and removed from the abdomen. The wounds are then closed.
Complications from gallbladder surgery are rare. Most patients will experience some pain post operatively, but this is to be expected and can be managed with pain killers.
Given the gallbladder is taken off the liver, some bleeding can occur. It is rare for the bleeding to be significant enough for a return the theatre.
Bile leaks occur in up to 2% of patients undergoing laparoscopic cholecystectomy. The symptoms usually occur within 1-2 days of surgery, and include ongoing pain, fevers, and a general feeling of being unwell. If this happens post operatively, the patient should been seen by the surgical team again.
A bile duct injury is an infrequent but significant complication of surgery. This is when the main bile duct is damaged. This can occur in 1:500 cholecystectomies, so is a rare complication. However, it is significant as would require more intervention and sometimes major surgery to correct.
Any keyhole procedure carries the risk of needing to converted to open surgery. This is when a cut is made in the abdomen, and the procedure is completed in an open fashion. The indications for this in gallbladder surgery would be if there was significant bleeding, abnormal anatomy and concern about causing damage by continuing a keyhole procedure. Open conversion is rare, happening in 1-2% of gallbladder surgery cases.